
Introduction
- A common indication for an ECG is in a patient presenting with acute chest pain or features suspicious for an acute coronary syndrome
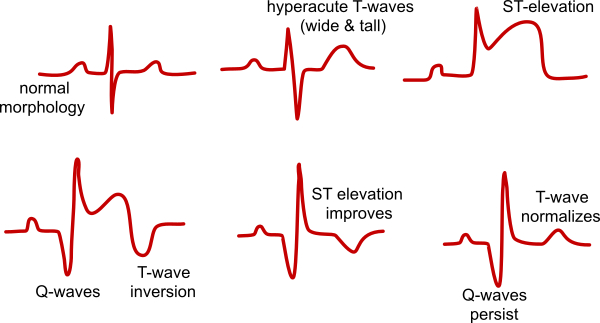
- The most important diagnosis to identify quickly is an acute ST elevation myocardial infarction (STEMI) because of its significant mortality rate and that urgent revascularisation may be indicated
- Any ST segment and T wave changes in a contiguous or geographical location of the heart may be consistent with myocardial ischaemia or infarction and should be considered carefully
- Be aware that acute coronary occlusion may be evolving or threatening despite normal ST/T changes
- A normal ECG does not rule out ischaemia or infarction. The nature of the pain, age and presence of risk factors and serum troponin also help risk stratify.
- Similarly ST/T changes can be seen in other acute and non-acute pathology and the rest of the ECG, clinical context and previous ECGs can help interpretation
- A critical therapeutic error occurs when thrombolysis or anticoagulation is administered by mistaking the ECG changes and chest pain of acute pericarditis or thoracic aortic aneurysm as a MI. Review the history carefully and consider additional testing before treatment
- The most frequent mistake by JMOs is to misinterpret the ST/T changes of bundle branch block, left ventricular hypertrophy and digoxin use as a myocardial injury pattern
CLASSIC STEMI PATTERNS
| ST/T changes | Other changes | Notes | |
| ST elevation myocardial infarction (STEMI) | Elevation in contiguous leads +/- ‘Reciprocal’ ST depression in other leads |
STEMI equivalents (High Risk)
| Wellen’s criteria (severe LAD disease) | Normal or mild ST elevation in contiguous leads Biphasic or deep T waves inversion |
History of resolved cardiac pain | |
| De Winter Waves (acute LAD occlusion) | Up-sloping ST depression and peaked T waves in antero-septal leads | ||
| Left Main Coronary Occlusion | Widespread ST depression especially lateral and high lateral leads ST elevation AVR |
||
| Hyperacute MI | Hyper-acute peaked T waves in contiguous leads | Repeat ECG after 10 minutes to identify evolving ECG changes | |
| Posterior myocardial infarction | ST depression in antero-septal leads | Dominant R wave and upright T waves in same leads Posterior leads show ST elevation |
Associated with hypotension if RV involvement |
Other STEMI
| Thoracic aortic dissection and RCA Occlusion | ST elevation in inferior leads | Sudden tearing chest pain radiating to inter-scapular region Do not thrombolyse |
Myocardial ischaemia (intermediate risk)
| Prinzmetal’s angina (coronary vasospassm) | Same as STEMI but spontaneously resolves | Normal biomarkers | |
| Myocardial ischaemia (pseudonormalisation) | Previously inverted T waves of old MI become upright during acute ischaemia | Check old ECG | |
| Non-STEMI (NSTEMI) | Depression in contiguous leads |
Non-specific (low risk)
| Intermediate risk | Downsloping ST segments or T wave flattening in contiguous leads |
ACS/STEMI mimics seen in acute pathology
ACS/STEMI mimics
Pre-existing structural cardiac disease
Very nice introduction about ECG in Chest Pain, Its helpful information. Thank you for sharing this useful information.